

Representation and Extrapolation: Evidence from Clinical Trials

What is this research about and why did you do it?
Economists have long recognized that innovation--while key to growth--does not benefit everyone equally. New technologies skew toward the wealthy (who are more profitable), and diffusion is faster in better-connected networks. This paper identifies and investigates a third cause of inequality in innovation: unrepresentative product testing can systematically erode trust within excluded populations. We investigate this hypothesis---that who is in the data matters for diffusion---in the context of medical innovation, where Black Americans make up 13% of the population, yet are less than 5% of clinical trial participants (with the modal trial for a new medicine enrolling zero; see NASEM report for further details)
How did you answer this question?
We develop a model of how people interpret data and pair it with a survey experiment of U.S. physicians and patients. In the theory, all individuals extrapolate more from data when they see themselves represented in it: evidence is viewed as more relevant and people update more readily, with diminishing returns to representation. We test these predictions by cross-randomizing medication efficacy with the demographic composition of patients in a (hypothetical) clinical trial for a new medication. We then measure how these features affect physicians’ beliefs about effectiveness for their patients and their willingness to prescribe the medication. We similarly randomize the efficacy and representation to Black and White patients, and query them on willingness to adhere to the medicine. Comparing responses across treatments provides a measure of how representation shapes updating on medical evidence and take-up of new technologies.
What did you find?
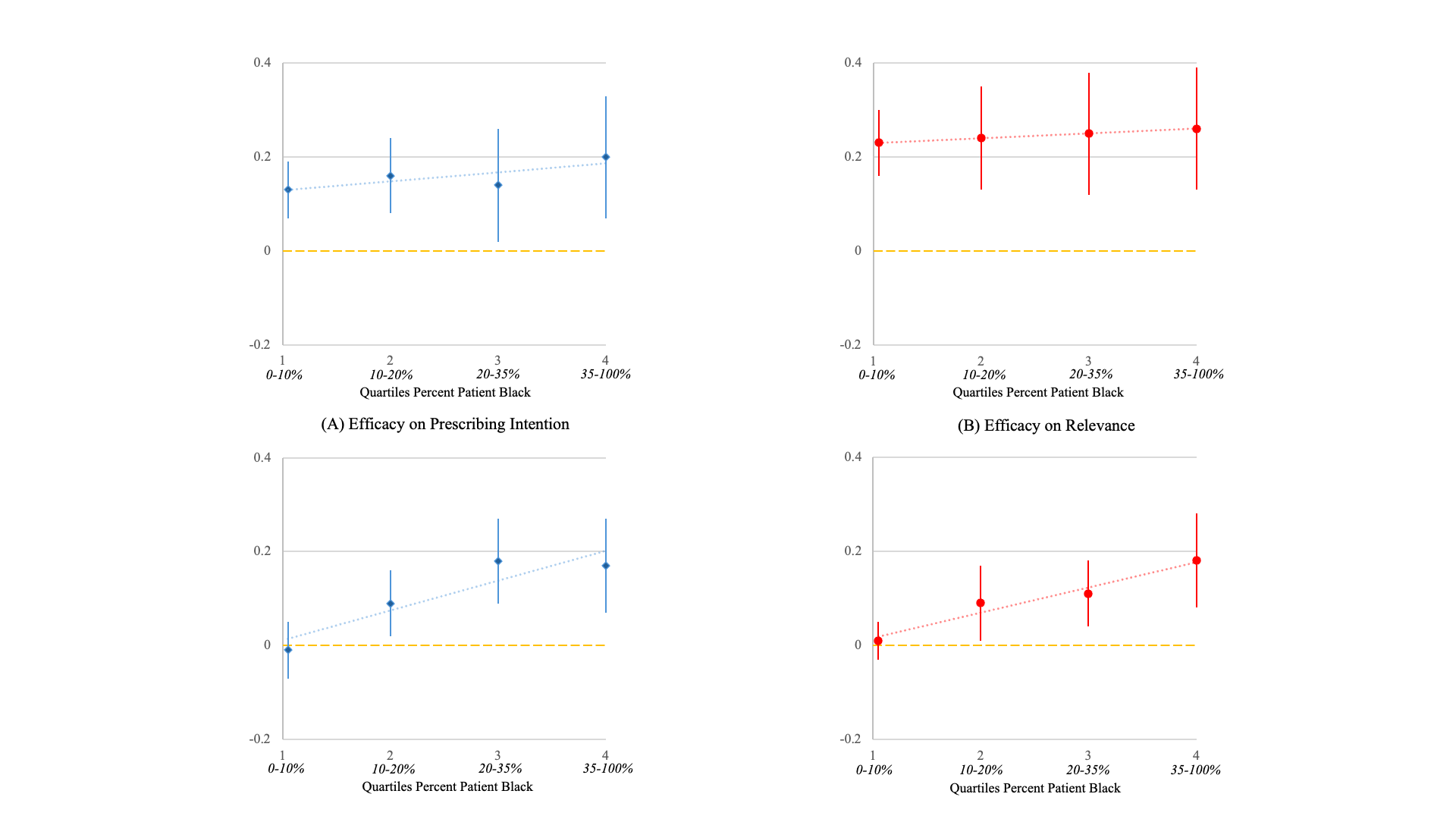
What implications does this have for the study (research and teaching) of wealth concentration or economic inequality?
The findings highlight a new mechanism through which inequality persists: when key inputs into decision-making (like data or evidence) are unrepresentative, learning is systematically tilted towards unequal adoption of beneficial technologies. It complements other work members of our research team have done on the importance of diversity in medical professionals (Alsan et al., 2019). For research, it underscores the importance of incorporating endogenous belief formation into models of inequality. For teaching, it emphasizes that who is included in data generation shapes outcomes, linking informational environments to the persistence of economic and health disparities.
Citation and related resources
Alsan, Marcella, Owen Garrick, and GrantGraziani. 2019. "Does Diversity Matter for Health? ExperimentalEvidence from Oakland." American Economic Review 109(12): 4071–4111.DOI: 10.1257/aer.20181446
Alsan, Marcella, Maya Durvasula, Harsh Gupta, JoshuaSchwartzstein, and Heidi Williams. 2024. “Representation and Extrapolation:Evidence from Clinical Trials.” Quarterly Journal of Economics 139 (1):575–635. https://doi.org/10.1093/qje/qjad036
National Academies of Sciences, Engineering, and Medicine.2022. Improving Representation in Clinical Trials and Research: BuildingResearch Equity for Women and Underrepresented Groups. Washington, DC: TheNational Academies Press.
https://www.youtube.com/watch?v=WylQEpEVnK4

-3sm.jpg)
.webp)

